

Writing a Useful Clinical History: What Your Pathologist Actually Needs to Know
The clinical history on a biopsy submission form is not a formality. It is, in many cases, the single most useful piece of information a pathologist receives. Tissue processed without context can still yield a diagnosis — but tissue accompanied by a complete, accurate clinical history yields a better one, faster.
This post is about what actually matters in that history, and why.
Why Clinical History Changes Diagnoses
Histopathology is pattern recognition constrained by probability. A pathologist assigning a diagnosis is not simply describing what is present microscopically — they are ranking possibilities given what is known about the patient, the lesion, and the clinical context. Two histologically similar lesions can carry entirely different diagnoses depending on species, site, signalment, and clinical course.
A classic example: a proliferative spindle cell lesion in the subcutis of a cat at a prior injection site carries a different differential list than an identical-appearing lesion in the subcutis of a dog. The tissue looks the same. The diagnosis is different. The pathologist cannot apply the right interpretive framework without knowing which patient they are looking at.
Clinical history does not bias the pathologist toward a predetermined answer. It gives them the tools to provide the right answer.
The Five Elements That Matter Most
1. Complete signalment
Species, breed, age, sex, and reproductive status. All five. Breed matters more than many clinicians appreciate — certain neoplasms and inflammatory conditions have strong breed predispositions that meaningfully shift differential rankings. Reproductive status is essential for any mammary, uterine, or prostatic lesion, and for conditions where hormonal status affects interpretation.
2. Lesion chronology
How long has the lesion been present? Has it changed — grown, ulcerated, regressed, recurred? Rate of growth is diagnostically informative. A mass that doubled in size over three weeks carries different implications than one that has been present and static for two years. If this is a recurrence, say so, and note the interval since the prior surgery.
3. Lesion characteristics at the time of excision
Size, location (be specific — "shoulder" is less useful than "dorsal scapular subcutis"), consistency, adherence to underlying structures, ulceration, and relationship to prior injection or trauma sites. If you inked the margins, indicate which color corresponds to which surface.
4. Prior treatments
Glucocorticoids, chemotherapy, radiation, and prior surgical excision all alter tissue histology in ways that can mimic or mask pathology. A lymph node with reactive hyperplasia in a dog two weeks post-dexamethasone looks different from one in an untreated dog. Topical treatments matter for skin biopsies. If the patient has been treated, include what was given, at what dose, and for how long.
5. Your differential list
This is not a test. You are not graded on whether your differential matches the pathologist's diagnosis. Sharing your clinical impression — even if uncertain — helps the pathologist understand the clinical problem you are trying to solve. If you are primarily ruling out neoplasia versus fungal granuloma in an immunocompromised patient, that context changes which special stains or ancillary tests might be worth recommending.
What the Pathologist Does With This Information
A complete history allows the pathologist to apply appropriate interpretive frameworks, recommend relevant ancillary testing proactively rather than reactively, phrase the diagnostic summary in clinically useful terms, and flag discordances between clinical and histologic findings — which are themselves diagnostically meaningful.
When a histologic finding does not fit the clinical picture, that discordance may indicate sampling error, an unusual presentation of a common disease, or a diagnosis the clinician had not considered. The pathologist can only flag it if they know what the clinical picture was.
A Note on Specificity vs. Length
A useful clinical history does not need to be long. It needs to be specific. "Skin mass, dog" is not a clinical history. "9-year-old intact female Golden Retriever, 2 cm firm, non-ulcerated subcutaneous mass, caudal aspect right forelimb, present approximately 3 months, slow growth, no prior treatment, DDX lipoma vs. soft tissue sarcoma" is a clinical history.
The difference in time required to write those two is under 30 seconds. The difference in diagnostic quality can be substantial.
Quick Reference: History Checklist
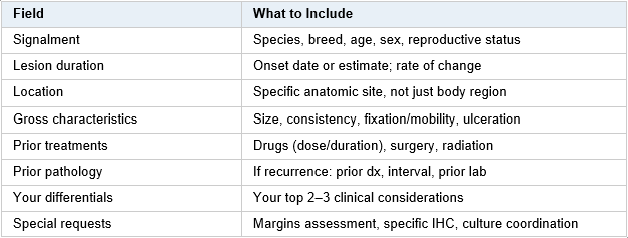
Short reference on the important features to include in a clinical history for biopsy or cytology submission.
If your submission form does not have fields for all of this, use the comments box. A pathologist reading a well-documented history is a better diagnostic partner than one working in the dark.
Eric Snook, DVM, PhD, DACVP — Vetopathy. Questions about submitting cases or optimizing your submissions? Reach out directly.