

Flow Cytometry for Lymphoma Immunophenotyping in Dogs and Cats: An Underutilized Tool
Lymphoma is one of the most common diagnoses in small animal oncology. It is also one of the most heterogeneous — a label that encompasses disease entities with meaningfully different biologic behavior, treatment responses, and prognoses. Flow cytometry is the tool that begins to resolve that heterogeneity at the time of initial workup, and it is commercially available right now through reference laboratories most practices already use.
Despite this, flow cytometry remains underutilized in general practice. The purpose of this post is to explain what it does, what it does not do, and when it should be part of your diagnostic plan.
What flow cytometry measures
Flow cytometry characterizes cells suspended in fluid by passing them through a laser beam and detecting light scatter and fluorescence signals from antibody-labeled surface markers. In the context of lymphoma workup, it identifies the immunophenotype of a lymphoid population — principally whether the neoplastic cells are of B-cell or T-cell origin, and whether they express markers consistent with a mature or immature differentiation state.
The key markers in routine veterinary lymphoma panels include CD3 (T-cell lineage), CD21 and CD79a (B-cell lineage), CD4 and CD8 (T-cell subsets), and CD34 (immaturity/blast marker). Additional markers such as MHC II, CD25, and CD11b extend the panel for specific subtypes. Commercial panels from IDEXX and Antech cover the core markers and are sufficient for the majority of clinical decisions.
Importantly, flow cytometry also evaluates clonality indirectly through aberrant antigen expression and abnormal scatter characteristics. This is distinct from PARR (PCR for antigen receptor rearrangement), which directly assesses clonality at the molecular level and is complementary rather than redundant.
Why immunophenotype matters clinically
The B-cell versus T-cell distinction in canine lymphoma is not academic. It carries direct prognostic and therapeutic implications that affect decisions made at the first oncology visit.
In dogs, high-grade B-cell lymphoma — the most common form, typically multicentric — responds well to CHOP-based protocols with median survival times of 12 to 14 months in favorable cases. High-grade T-cell lymphoma carries a substantially worse prognosis, with median survival times often under six months on the same protocols. This difference is large enough that most oncologists require immunophenotype prior to discussing treatment goals and client expectations.
T-zone lymphoma (TZL) is a low-grade T-cell lymphoma with a distinctive flow cytometry profile — small CD3+/CD4+/MHC II-negative lymphocytes — and a markedly better prognosis than high-grade T-cell disease, with many dogs surviving two or more years without chemotherapy. Flow cytometry is the primary tool for identifying TZL, and its recognition changes management completely. A dog with TZL and an owner who cannot pursue chemotherapy is in a very different situation than a dog with high-grade T-cell lymphoma in the same circumstance.
In cats, the B- versus T-cell distinction carries less dramatic prognostic weight than in dogs, but immunophenotype remains relevant for subtype classification and for distinguishing lymphoma from reactive lymphoid hyperplasia, particularly in the context of alimentary disease where small cell lymphoma (T-cell, indolent) and large cell lymphoma (B- or T-cell, aggressive) require fundamentally different treatment approaches.
Sample requirements and practical considerations
Flow cytometry requires viable cells in suspension and is therefore ideally performed on fresh, unfixed material. Lymph node fine needle aspirates submitted in saline or RPMI transport medium are the most common sample type. Peripheral blood is appropriate when circulating neoplastic lymphocytes are suspected — leukemic phase lymphoma or chronic lymphocytic leukemia. Bone marrow can also be submitted for staging.
The critical practical point: flow cytometry cannot be performed on formalin-fixed tissue. It is a companion test to histopathology, not a substitute for it. The workflow for a dog with suspected multicentric lymphoma should include cytology or histopathology for morphologic assessment and flow cytometry for immunophenotyping, ordered concurrently rather than sequentially.
Turnaround time at major reference laboratories is typically 24 to 72 hours from sample receipt, which does not meaningfully delay treatment initiation in most cases.
Flow cytometry vs. PARR: which to order
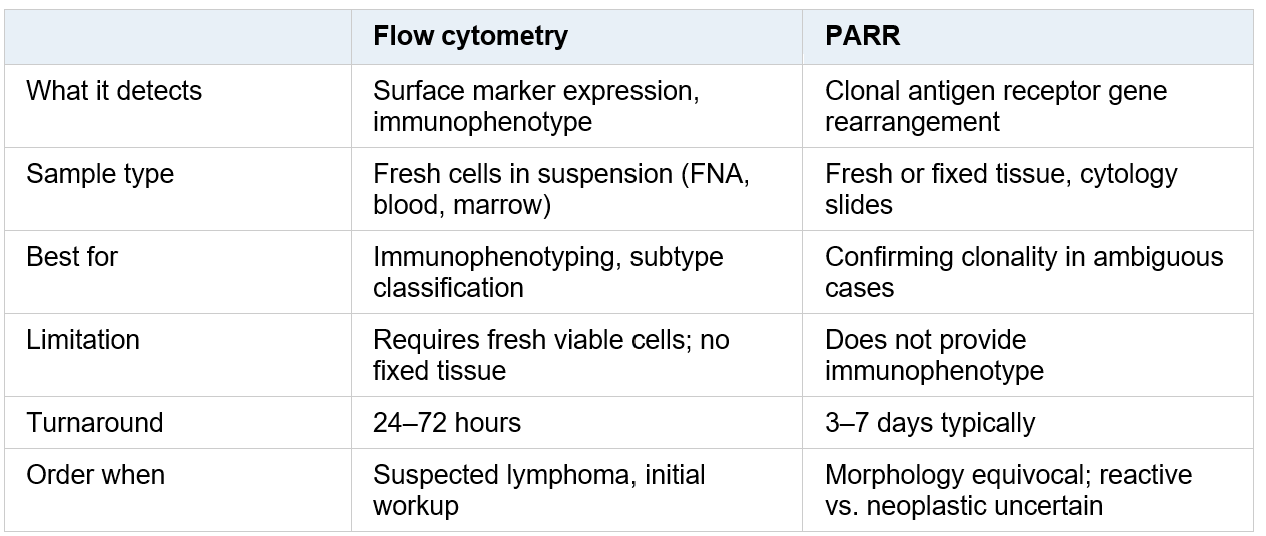
This table demonstrates when flow cytometry or PARR are most useful for diagnosing lymphoma and what is required for each test.
In practice, flow cytometry is the first-line ancillary test for most lymphoma workups. PARR is most useful when the cytologic or histologic picture is ambiguous and the question is whether a lymphoid proliferation is reactive or neoplastic, or when flow cytometry results are inconclusive.
When to include flow cytometry in your plan
Any dog or cat with peripheral lymphadenopathy, a mediastinal mass, splenomegaly with lymphoid infiltrate, or alimentary disease with suspected lymphoid neoplasia is a candidate for flow cytometry. The test adds meaningful information whenever immunophenotype will influence prognosis communication, treatment selection, or the decision about whether to pursue further workup.
It is not indicated as a standalone test when histopathology has already established a specific lymphoma subtype with sufficient morphologic and architectural detail — in those cases, immunophenotype may already be inferable or confirmable by IHC on the fixed tissue. But in the early workup phase, when you are working from cytology and the question of B versus T has not yet been answered, flow cytometry is the fastest path to that answer.
The bottom line
Flow cytometry for lymphoma immunophenotyping is not an emerging technology. It is available and clinically actionable today. The B- versus T-cell distinction, the recognition of T-zone lymphoma, and the identification of leukemic phase disease are all within reach of a well-ordered initial workup. The cases where this information does not matter are fewer than the cases where it does.
If flow cytometry is not currently part of your lymphoma workup protocol, it is worth revisiting why — and whether the answer still holds.
Eric Snook, DVM, PhD, DACVP — Vetopathy. Flow cytometry results can be integrated with histopathologic findings for a complete lymphoma workup. Inquiries welcome.