

Acanthomatous Ameloblastoma: When the Margins Tell the Real Story
Case Spotlight · Canine · Oral Pathology, Oncology
Canine acanthomatous ameloblastoma is one of the better-known oral tumors in small animal practice — locally aggressive, radiographically osteolytic, and with a prognosis that hinges almost entirely on the adequacy of surgical margins. This case illustrates several aspects of the diagnostic and surgical workflow that are worth examining: the two-step biopsy-then-referral sequence, what radiographs can and cannot show, and why narrow margins in a markedly invasive tumor require honest prognostic framing regardless of what the numbers say.
Signalment and presentation
The patient was an 11-year-old spayed female pit bull mix presenting to a veterinary dental specialist for evaluation of a gingival mass. The mass measured 11 x 8 mm and was associated with the buccal and mesial aspects of tooth 307 (mandibular left second premolar). It was described as red and firm on oral examination.
This was not the first encounter with this lesion. The mass had previously been biopsied by the primary veterinarian, and that initial biopsy had returned a diagnosis of canine acanthomatous ameloblastoma (CAA). The referral to the dental specialist was specifically for definitive surgical management — rim excision including teeth 306 through 308 — with a request to evaluate margins on the excised specimen. This two-step workflow — biopsy first, surgical referral second — is the appropriate sequence for oral masses where the diagnosis will determine the surgical approach, and this case followed it correctly.
A note on the radiographic findings
Dental radiographs obtained at the time of the specialist visit showed no visible bone loss associated with the mass. This is a finding worth pausing on, because CAA is defined in the literature by its consistent invasion of adjacent cortical bone — osteolysis on radiographic evaluation is described as a characteristic feature of the tumor.
The absence of radiographically visible bone loss does not mean bone was uninvolved. CAA invades bone early and aggressively, but early cortical involvement may not produce radiographically detectable changes until a threshold of bone destruction has been reached. Microscopic invasion of bone can be present and histopathologically confirmed before it is visible on any imaging modality. This case reinforces a principle that applies broadly in oral oncology: radiographic findings set a floor, not a ceiling, for the extent of disease. The histopathologic assessment of the resected specimen is the more sensitive measure of true local extent.
Histopathologic findings and margin assessment
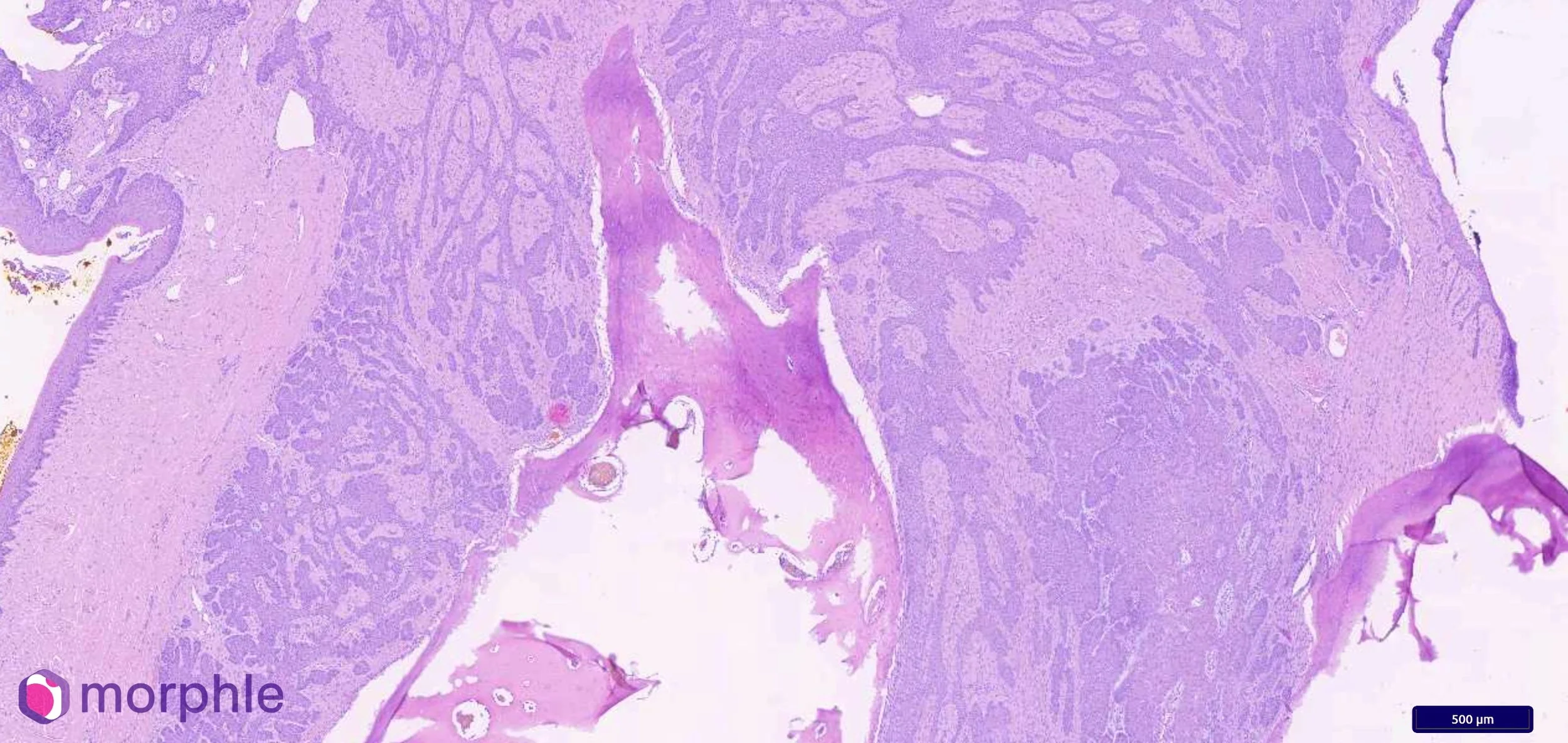
Sections of the excised gingival mass demonstrated an infiltrative, densely cellular, poorly demarcated nodular neoplasm. Neoplastic cells were arranged in trabeculae and islands within a fine fibrovascular stroma. The cells were polygonal with a moderate amount of eosinophilic cytoplasm and distinct cell borders, with round nuclei and finely stippled chromatin. Two features were particularly prominent: intercellular junctions — a reflection of the epithelial origin of the tumor — and peripheral palisading of neoplastic cells at the margins of the cellular islands. The mitotic count was low at 1 per 2.37 mm², consistent with the generally indolent proliferative behavior of CAA despite its local aggressiveness. The diagnosis was confirmed: canine acanthomatous ameloblastoma.
Margin assessment was performed on additional tissue sections following initial processing. The deep margin measured approximately 3 mm and the nearest lateral margin approximately 4 mm. The overall assessment: narrowly excised.
Three and four millimeters are not zero. In many tumor types these margins would be considered acceptable or even comfortable. In CAA, they require careful interpretation. The published literature, including the landmark Goldschmidt et al. series of 264 dogs (J Vet Dent, 2017), establishes that adequate surgical excision of CAA requires a minimum 1 cm margin of grossly and radiographically normal bone and soft tissue. Recurrence rates below 20% are achievable with adequate margins; incomplete or narrow excision carries substantially higher recurrence risk.
Beyond the measured distances, the tumor itself was markedly invasive — sending thin infiltrative projections along fascial planes and between bone trabeculae that extend beyond the visible tumor mass and beyond what any single plane of histologic section will capture. A margin that measures 3 mm in evaluated sections may be 0 mm in a plane those sections did not pass through. Narrow margins in a markedly invasive tumor are not the same as narrow margins in a well-circumscribed lesion. The recommendation for monitoring for recurrence is a specific instruction grounded in the tumor's biology, not a formality.
The rim excision: surgical approach and its implications
The surgical approach in this case was rim excision — removal of the gingival mass with a surrounding cuff of normal tissue including the adjacent teeth (306–308), preserving mandibular continuity. Rim excision is appropriate for CAA when the tumor is small, located in a site where adequate margins can be achieved without segmental mandibulectomy, and when preoperative imaging does not suggest deep medullary bone involvement. It is a less morbid procedure than segmental mandibulectomy and carries excellent functional outcomes when margins are adequate.
The tradeoff is that rim excision is a margin-sensitive procedure. The depth of bone removal is limited by the need to preserve mandibular continuity, and in a tumor that invades bone aggressively and sends microscopic projections beyond the visible mass, the achievable margin depth may be constrained by anatomy. This case illustrates that tension directly: the surgical approach was appropriate for the tumor size and location, and the resulting margins — while narrow — reflect the limits of what rim excision can achieve in this anatomic context rather than a technical error.
CAA: behavior, prognosis, and what makes this tumor unusual
Canine acanthomatous ameloblastoma occupies an unusual position in the oral tumor landscape. It is locally aggressive in a way that rivals malignant tumors — consistent bone invasion, high recurrence risk with incomplete excision, and a growth pattern that defies easy containment — yet it does not metastasize. Regional lymph nodes and distant sites are not at risk. The disease is entirely local, and the prognosis with adequate surgery is excellent.
This combination of local aggression without metastatic potential means that the entire prognostic weight falls on the surgical margin. There is no staging workup for distant disease, no chemotherapy indication, no radiation as an alternative to surgery in most cases. The question is simply: was the excision adequate? And if not, will the tumor recur, and can it be managed at recurrence?
Recurrence after narrow-margin excision is not uniformly catastrophic. CAA that recurs is generally amenable to re-excision, and some dogs undergo multiple procedures with prolonged disease-free intervals. The cumulative morbidity of repeated oral surgeries is a consideration, particularly in an 11-year-old patient, but CAA is not a diagnosis that closes the door on long-term quality outcomes. Monitoring for recurrence is the appropriate clinical instruction and reflects a realistic, not pessimistic, assessment of where this case stands.
Clinical takeaways
Several principles from this case are worth carrying into the next oral mass workup. Biopsy before surgery — the two-step sequence followed here — is the correct approach for any oral mass where the diagnosis will determine the surgical plan. Attempting definitive excision of an undiagnosed oral mass without prior histopathologic diagnosis risks either under-excising a tumor that needed wider margins or over-excising a lesion that did not warrant aggressive surgery.
Radiographic absence of bone loss does not exclude bone invasion in CAA. Histopathology of the resected specimen is the definitive assessment of local extent, and the pathology report should be read with that understanding.
Narrow margins in a markedly invasive tumor are not equivalent to narrow margins in a well-circumscribed lesion. The invasive architecture documented in the pathology report is clinically meaningful information that should directly inform the monitoring plan.
Case diagnosed by Eric Snook, DVM, PhD, DACVP — Vetopathy. All patient and clinician details anonymized. Oral pathology submissions evaluated with margin assessment and breed-specific context as standard practice.